By Dr Priya Rathi, Pain & Spine Specialist
Persistent lateral elbow or dorsal forearm pain is commonly misdiagnosed as tennis elbow. In a subset of patients, the actual cause is posterior interosseous nerve (PIN) entrapment, a motor nerve compression syndrome that is frequently missed because routine imaging is often normal.
Correct diagnosis is essential, as treatment and outcomes differ significantly from common elbow tendinopathies.
Understanding the Posterior Interosseous Nerve
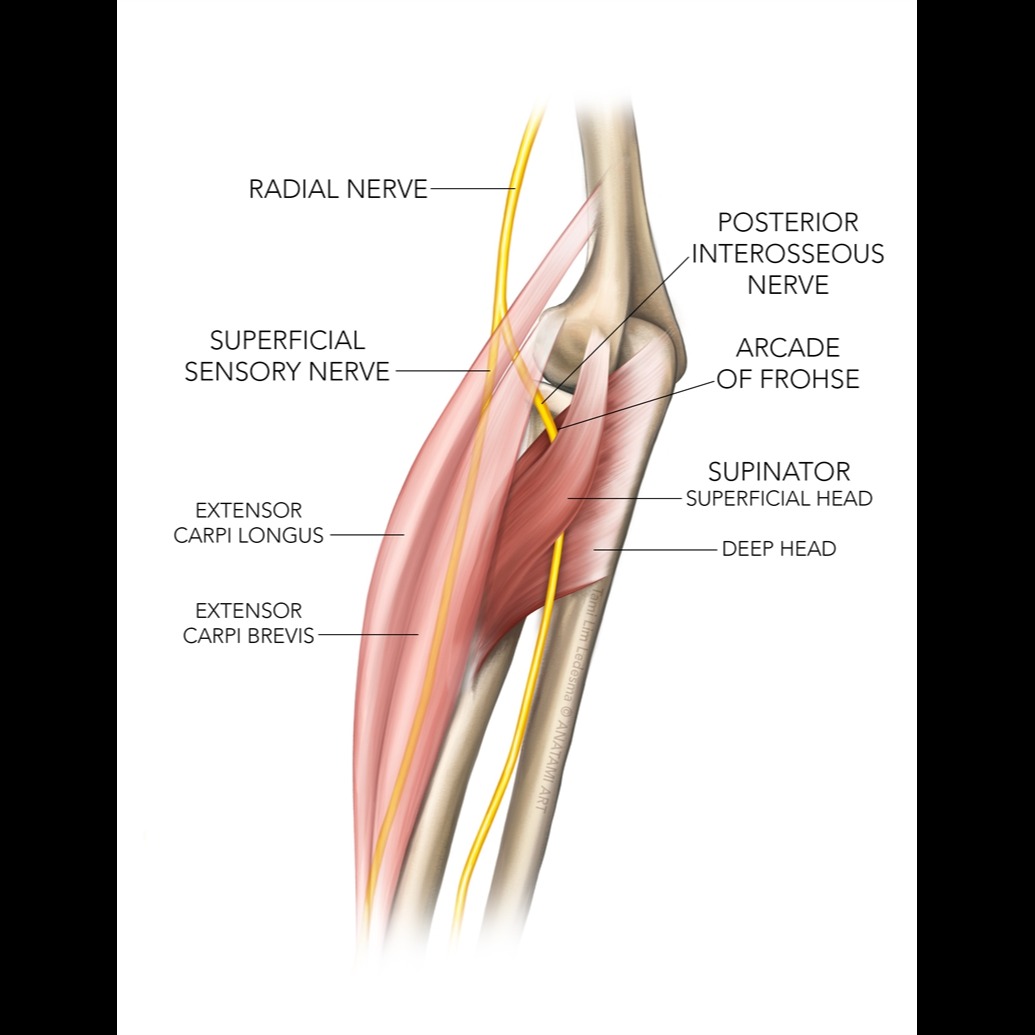
The posterior interosseous nerve is the deep motor branch of the radial nerve. It passes through the radial tunnel and enters the forearm by traversing the supinator muscle, which is the most common site of entrapment.
Importantly, the PIN does not supply sensation and does not innervate the primary wrist extensors.
Causes of Posterior Interosseous Nerve Entrapment
PIN entrapment commonly occurs due to:
• Compression within the supinator muscle
• Repetitive forearm rotation and overuse
• Chronic muscle tightness and fibrosis
• Post-traumatic scarring
• Long-standing untreated lateral elbow pain
Muscle-related compression is a major but under-recognized contributor.
Symptoms of PIN Entrapment (Clinically Correct)
Patients may present with:
• Deep, poorly localized pain in the lateral elbow or proximal forearm
• Pain worsened by forearm rotation or resisted finger extension
• Weakness of finger and thumb extension
• Difficulty straightening fingers or thumb
• Preserved wrist extension, sometimes with radial deviation
• No sensory symptoms such as numbness or tingling
In early or pain-dominant stages, weakness may be absent and pain is the primary complaint.
How PIN Entrapment Differs from Tennis Elbow
• Pain is deeper and more diffuse
• Local tenderness over the lateral epicondyle may be minimal
• Physiotherapy focused only on tendons often fails
• Imaging studies are usually normal
Failure to recognize this leads to prolonged suffering and unnecessary treatments.
Diagnosis of Posterior Interosseous Nerve Entrapment
Diagnosis is primarily clinical, supported by targeted evaluation.
At our pain clinic, assessment includes:
• Detailed history with activity correlation
• Focused neuromuscular examination
• High-resolution musculoskeletal ultrasound to assess nerve course, muscle compression, and dynamic entrapment
• Diagnostic nerve blocks when required
Normal MRI or X-ray does not rule out PIN entrapment.
Non-Surgical Management of PIN Entrapment
Most patients respond well to precise, non-surgical pain management when the true pain generator is addressed.
Ultrasound-Guided Dry Needling
Ultrasound-guided dry needling of the supinator and surrounding forearm muscles helps relieve muscle-induced nerve compression, improves local circulation, and reduces nerve irritation with high accuracy.
Ultrasound-Guided Nerve Blocks
Selective posterior interosseous nerve blocks help reduce inflammation and confirm diagnosis while providing pain relief.
Injection-Based Pain Therapies
In chronic cases with fibrosis or persistent inflammation, targeted injections may be used to break the pain cycle.
Pain-Focused Activity Modification
Rehabilitation guidance is individualized to avoid aggravating nerve compression rather than applying routine strengthening exercises prematurely.
Role of Surgery
Surgical decompression is rarely required and is considered only when:
• There is progressive motor deficit
• Symptoms persist despite well-directed non-surgical treatment
• Structural compression is clearly identified
Early referral to a pain specialist can often prevent surgery.
Why Early Pain Specialist Evaluation Matters
Posterior interosseous nerve entrapment is often missed because it does not fit classic orthopedic patterns and does not show clearly on scans. A pain-focused, muscle-and-nerve-based approach allows early diagnosis and effective non-surgical treatment.
Key Takeaway
Posterior interosseous nerve entrapment causes finger and thumb extension weakness with preserved wrist extension and no sensory loss. Recognizing this distinction is critical for correct diagnosis and successful management.